A client reports that she has a femoral artery stent, placed in 2017. Her doctor and nurse think massage is fine. All systems go, right? Maybe, maybe not. It turns out this topic is a lot more controversial than we knew, and a lot depends on what kind of stent she got.
Resources:
Pocket Pathology: /abmp-pocket-pathology-app
Adlakha, S. et al. (2010) ‘Stent fracture in the coronary and peripheral arteries’, Journal of Interventional Cardiology, 23(4), pp. 411–419. doi:10.1111/j.1540-8183.2010.00567.x.
Al-Nouri, O. et al. (2012) ‘Failed superficial femoral artery intervention for advanced infrainguinal occlusive disease has a significant negative impact on limb salvage’, Journal of Vascular Surgery, 56(1), pp. 106–111. doi:10.1016/j.jvs.2011.10.108.
Angioplasty and stent placement - peripheral arteries - discharge : MedlinePlus Medical Encyclopedia (no date). Available at: https://medlineplus.gov/ency/patientinstructions/000234.htm (Accessed: 5 April 2022).
Angioplasty and stent placement - peripheral arteries: MedlinePlus Medical Encyclopedia (no date). Available at: https://medlineplus.gov/ency/article/007393.htm (Accessed: 5 April 2022).
Cerino, V., July 15, U. public relations |, and 2015 (2015) Researchers study failed stents for peripheral artery disease, University of Nebraska Medical Center. Available at: https://www.unmc.edu/news.cfm?match=17216 (Accessed: 5 April 2022).
How Do Stents in Legs Help Unblock Arteries to Treat PAD? (no date). Available at: https://www.webmd.com/heart-disease/what-to-know-stents-legs-peripheral-artery-disease (Accessed: 5 April 2022).
Kerr, H.D. (1997) ‘Ureteral stent displacement associated with deep massage’, WMJ: official publication of the State Medical Society of Wisconsin, 96(12), pp. 57–58.
Martin, R. et al. (2021) ‘Common Femoral Artery Stenting: Computed Tomography Angiography Based Long-Term Patency’, Journal of Vascular Surgery, 74(2), p. 676. doi:10.1016/j.jvs.2021.05.003.
Peripheral Vascular Stent Insertion: Background, Indications, Contraindications (no date). Available at: https://emedicine.medscape.com/article/1839716-overview (Accessed: 5 April 2022).
Schillinger, M. and Minar, E. (2009) ‘Past, present and future of femoropopliteal stenting’, Journal of Endovascular Therapy: An Official Journal of the International Society of Endovascular Specialists, 16 Suppl 1, pp. I147-152. doi:10.1583/1545-1550-16.16.I-147.


0:00:01.2 Speaker 1: Hey, I have a client who listeners, did you know I have a growing library of NCB approved one-hour online self-paced continuing education courses that you can do any time, anywhere. Well, now you know, current classes include what's next COVID 19 updates from massage therapists and a massage therapist's, Introduction to pharmacology part one, and brand new, a massage therapist's Introduction to pharmacology part two, classes are $20 each, and they confer one hour of continuing education credit. Wanna know more? Visit my website @ ruthwerner.com and check it out. Be sure to sign up for my mailing list so you'll never miss a new class. Anatomy trains is delighted to invite you to our in-person fascial dissection workshop, May 30th through June 3rd, 2022. We're excited to be back in the lab with Anatomy Trains, author Tom Myers and master dissector Todd Garcia in Todd's laboratory of anatomical enlightenment in Boulder, Colorado. Join students from around the world and from all types of manual movement and fitness professions to explore the real human form, not the images you get from books. Visit anatomytrains.com for details. Hi, and welcome to I have a client who pathology conversations with Ruth Werner, the podcast where I will discuss your real life stories about clients with conditions that are perplexing or confusing.
0:01:47.2 S1: I am Ruth Werner, author of a massage therapist's Guide to pathology, and I have spent decades studying, writing about and teaching about where massage therapy intersects with diseases and conditions that might limit our client's health, we almost always have something good to offer even with our most challenged clients, but we need to figure out a way to do that safely, effectively and within our scope of practice, and sometimes as we have all learned... That is harder than it looks.
0:02:20.1 S1: Today's story comes from a massage therapist who contacted me via my Facebook page, Ruth Werner's pathology page, and in Facebook messenger, she left me this... Ruth, I was wondering if you have any information on stents in the legs. The stent was done in 2017, the doctor gave her clearance for massage, I was just concerned with a stent in the leg and if massaging the leg could do any harm, I talked to the doctor's nurse, she said it would be okay. I have never worked on anyone with a leg stent, to tell you the truth, I'm a little nervous of this, I've been practicing for 22 years, I have never run across this in my practice, the client is now 70 years old. If a stent is in the leg... Can you palpate it? I don't wanna cause any harm. Do you think doing any leg work should be avoided? PubMed has some articles on massage with Stent, deep tissue is contraindicated in the area, I asked on the massage therapist Facebook page, and they had mixed comments, not many have worked with leg stents.
0:03:24.7 S1: I'm leaning on saying no. Well, listeners, I had some fun with this topic and I discovered some things that I wasn't expecting, and they might or might not be relevant to this particular case, but they could apply to a lot of other people who have had femoral artery stents, and it's not the kind of thing you might find with just a superficial glance at this topic, but before we get to all of that, let's talk a little bit about peripheral artery disease, you're probably familiar with atherosclerosis, and this is the condition where deposits of fat, calcium, fibrous tissue, other stuff, can build up in the arteries, and this happens, especially where blood pressure is really high, or where there's a lot of friction, or where blood gets pushed around sharp corners or in areas where arteries bifurcate so there's a lot of turbulence just at that fork in the road, and usually when we talk about atherosclerosis, it's in relation to arteries near the heart or in the neck, we talk about atherosclerosis of the coronary arteries, that's coronary artery disease.
0:04:43.1 Speaker 2: Atherosclerosis can develop in the aorta and less commonly among some other abdominal arteries, and atherosclerosis is pretty common in the carotid arteries, those are the arteries of course, that supply our brain with blood, and we call that carotid artery disease, but sometimes atherosclerotic plaques can develop in arteries that are not in the trunk, and when this happens, we call it peripheral artery disease, very rarely, this might happen in the arms, but it's not that uncommon to see peripheral artery disease occur in the legs and the artery in the legs that is most likely to be affected is the superficial femoral artery. Who gets peripheral artery disease, well, it's pretty much the same population of people who get other kinds of atherosclerosis, and that gives us some hints about this client, the fact that she has this history with her leg suggests she may also be dealing with cardiovascular disease in other locations, and that could be important information to gather...
0:05:24.7 S1: Of course, and we'll come back to that later. Signs and symptoms of peripheral artery disease include a thing called claudication that's C-L-A-U-D-I-C-A-T-I-O-N. That's severe cramping pain that might come up during exercise, but we might also see weakness or numbness in the legs, coldness in the lower leg or the foot, sores on the feet or the legs or the toes, weak or no pulse in the legs or the feet, and a blocked artery can increase the risk of developing serious infections, including gangrene, and that can lead to a need for amputation.
0:06:27.2 S2: Yikes, right. So what do we do about peripheral artery disease, when an artery that supplies the leg or the heart or the head or whatever it is, is occluded with atherosclerotic Plaque, it can be repaired, this used to be done often with open surgery to snip out the affected portion of the artery and stitch in a replacement piece or with open surgery to remove the affected part of the artery and then stretch the ends and stitch those back together, but of course, these interventions are extremely complicated with lots and lots and lots of risks.
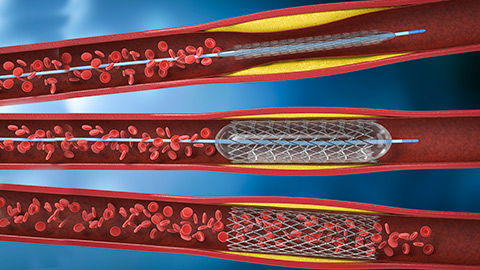
0:07:24.7 S1: That's why the advent of endovascular procedures has been so important, I'm sure you've heard of balloon angioplasty, if you take that apart, you can see it means reshaping blood vessels by using a balloon. What happens in a balloon angioplasty is that a long, thin, very flexible catheter is threaded through a major artery to the site of blockage, and when that catheter has reached that blocked up point, then a tiny balloon is inflated to stretch the walls of that occluded artery, and then in some situations, a stent that is a piece of tubing that could be made of various kinds of materials is inserted into the affected section of artery, and that has the intention of keeping it all open, then the catheter and the balloon are withdrawn and the stent stays in place, some stents also slowly release medications that help keep them open and clot-free the body eventually builds scar tissue around it, so that the stent is stable and permanent, and that little bit of tubing is supposed to keep that section of artery open forever.
0:08:15.9 S1: Now, this strategy for femoral artery stenosis is fairly recent, that is just within the last 30 years or so before then. The typical treatment for peripheral artery disease was open surgery, which as we talked about, has all kinds of risks, so now we often see balloon angioplasty and the insertion of a stent in the femoral artery, and this appears to be what our client for today has had happen. So let's talk about her. She's 70 years old. Her stent was placed in 2017. It's been there for five years. She'd like to receive massage. Her doctor says it's okay. Her doctor's nurse says it's okay, and yet I will say there are still a few things we need to know specifically about her health in general, and about her cardiovascular health in particular, but also about her general activity levels beyond these... At this moment, I couldn't see any really serious reasons why not to offer massage therapy with the caveat that we don't go poking or prodding or pushing intrusively in the area where the stent was inserted, instead we might treat that leg with some extra care and caution including it in the massage, but not making it a special point of focus, but wait, because there's more...
0:09:37.3 S1: It turns out that endovascular procedures for femoral artery occlusions are somewhat controversial, and this is because at least until very recently, this surgery had a surprisingly high failure rate. Here's a little tidbit I found, this is paraphrased from a 2010 paper called stent fracture in coronary and peripheral arteries, and it goes like this, "Inherent risks of stenting include re-stenosis and thrombosis, recently stent fractures have been recognized as a complication that may result in thrombosis, perforation, re-stenosis and migration of the stent resulting in morbidity and mortality, stent fractures were originally seen in the superficial femoral arteries, but have since then been reported in almost all vascular sites, including the coronary, renal carotid, iliac and femoral popliteal arteries, fractures are the result of the complex interplay between stent manufacturing the stented segment PosiTile and non-PosiTile biomechanical forces and plaque morphology at the particular vascular site, despite being recognized as an important complication consensus on routine surveillance and diagnostic methods to detect stent fractures continues to be lacking.
0:11:24.7 S1: Fortunately, most cases are relatively benign and can be managed conservatively if detected in a setting of recurring symptoms, further intervention is usually sought". Well, to me, that sounds really alarming, these stents, especially in the superficial femoral artery seem to fracture and pretty readily, and we don't have Good best practices systems in place to track that early, and this finding is supported by another paper that followed patients for three years from 2007 to 2010, and there were, I believe there were 39 patients who had had a total of 42 stents put in, and among these patients over half of the stents needed to be completely replaced within the first year, and they also found that outcomes were much better for patients whose peripheral artery disease was less severe when a stent was first inserted, and there's a lesson in that as well, and of course, all these references are in your show notes, to me, this all sounds pretty dire, and it doesn't help that...
0:12:18.3 S1: Here is the list of possible risks as published by several websites that advertise femoral stents, the risks include an allergic reaction to the drug used in a stent that releases medicine into your body, an allergic reaction to x-ray dye, bleeding or clotting in the area where the catheter was inserted, blood clots in the legs or the lungs, damage to the blood vessel, damage to a nerve which could cause pain or numbness in the leg, damage to the artery in the groin, which might need urgent surgery, heart attack infection at the surgical cut. Kidney failure, misplacement of the stent, stroke failure to open the affected artery and loss of limb.
0:13:01.9 S1: Gosh, that's a lot. I wanna give a really good shout out to our contributor who also did some digging of their own, and they shared with me a 1997 case report in which massage was inferred to have caused the dislocation and migration of a stent. Very alarming, of course, this paper is in your show notes, but it's a bit of a different situation because in this situation, the massage was deep roll thing and the stent was in a ureter not in The superficial femoral artery, the patient was fine by the way, but there's a good takeaway lesson here too, don't work intrusively in areas where we know stents have been inserted, add to this everything we've just learned about those seemingly fragile femoral artery devices that in my mind's eye at least just seem to be waiting for an opportunity to fail.
0:13:58.1 S1: And it seems like this massage therapist's concerns are totally justified, and maybe this is a client who just isn't a good candidate for leg massage, however, I do have some good news, there have been some recent innovations in stent manufacturer and the materials appear to have made them much more stable and functioning for the long-term, this client with her 2017 surgery probably got one of the newer versions of leg stents, that said, I would be really interested to know if she's needed any follow-up care for her stent or if it causes any particular symptoms or side effects for her, when we have that information plus ideas about her overall cardiovascular health or her activities of daily living, then we can be in a position to be maybe cautiously optimistic about massage for her. This was a really tangley situation, a leg stent. Okay, seems like just a local caution, right, but then it turns out that stents can sometimes be really fragile, so maybe we better avoid them all together, but now with better technology, we might be back to just a local caution, depending on those other health-related variables. I really appreciate this massage therapist's concerns and certainly would not quibble with the decision to not do massage on this person's legs, but I think that with care and conservatism they could probably move forward at least enough to incorporate...
0:15:30.8 S1: That's one of my favorite body work words, to weave the Corp or the body all together to incorporate this part of the body, the legs, with the rest of the beloved Whole. I'm interested in your thoughts on what you just learned about superficial femoral artery stents and about your I have a client who stories. So let's be in touch.
0:15:55.0 S1: Hey everybody, thanks for listening to I have a client who pathology conversations with Ruth Werner. Remember, you can send me your I have a client who stories to ihaveaclientwho@abmp.com that's ihaveaclientwho all one word, all lowercase @abmp.com. I can't wait to see what you send me and I'll see you next time.