





Most of us who’ve done massage for a while have at some point during a session elicited a jump reflex or yelp as an elbow or sharp fingertips accidentally landed on a client’s nerve. Normally, we reposition our contact point to avoid the sensitive area, but not always. During my first couple years in practice, I thought the client’s pain reflex might be a sign that I’d discovered the problematic area. Finally, I began to suspect that my attempts at “chasing the pain” may have been chasing off some of my clients. Here, I’ll discuss the top three nerves that have given me the most trouble and demonstrate myoskeletal techniques for avoiding these sensitive areas.
Sciatic Nerve
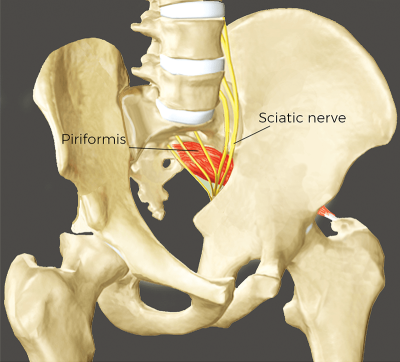
The bulky sciatic nerve isn’t the only neural structure traversing through the greater sciatic notch, but it’s the one I’ve probably aggravated the most, especially when treating clients with piriformis syndrome (Image 1). A misplaced elbow with the client prone can easily trigger pain and may even bruise the nerve if forcefully or repetitively compressed against the ischial spine. Random poking on the nerve can trigger sharp, radiating pain and, in some cases, numbness and accompanying gait alterations.
I finally discovered I could avoid bullying the sciatic nerve by treating the client in a sidelying position. The first step in this routine is to flex the client’s knees and trunk to 90 degrees. In this posture, the piriformis changes from an external to internal hip rotator (and abductor) due to its insertion on the superior border of the greater trochanter. The therapeutic benefit of this flexed position is that it tautens the piriformis muscle, allowing greater forearm contact and more precise assessment for tightness and spasm.

and work the piriformis insertion at the greater trochanter.
In Image 2, my ulna bone pressure is focused on the piriformis tendinous insertion at the greater trochanter. I begin by allowing my soft forearm to slowly sink into the tendon. Once I feel I have a good tissue hook, I ask the client to begin a slow and rhythmic pelvic rocking motion. By hooking and dragging the piriformis tendon inferiorly as the client’s hip attempts to move superiorly, I can trigger a Golgi tendon organ release, causing the muscle to loosen its grip on the sciatic nerve.
Cervical Nerve Roots
For years, my go-to routine for addressing anterior scalene tightness in clients presenting with thoracic outlet syndrome was to get them supine and use my fingers to wade through the anterior neck, palpating for tightness at the muscle’s origin at the transverse processes (C2-C6) or insertion at the first rib. Even with years of practice, my fingertips would sometimes stray to a nearby nerve root and cause discomfort. One day, while teaching a class in Costa Rica, I was helping a participant whose partner was in a sidelying position and it suddenly occurred to me that I might have better and safer scalene access by entering through the lateral side of the neck rather than going in from the front.

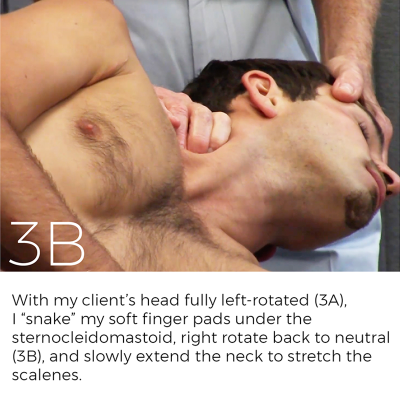
Notice in Image 3A how the technique begins with my client’s head fully left-rotated. This allows me to “snake” my soft finger pads under the sternocleidomastoid. Then I right rotate the client’s head back to neutral and slowly extend the neck while my soft fingertips gently resist by pinning the scalenes to bone (Image 3B). I love this technique, and I’ve never had trouble intruding on the nerve roots or vascular structures. It’s a bit tricky at first, so I recommend practicing it in a supervised setting.
Superior Cluneal Nerve
nerves where they pass over the bony pelvic brim.
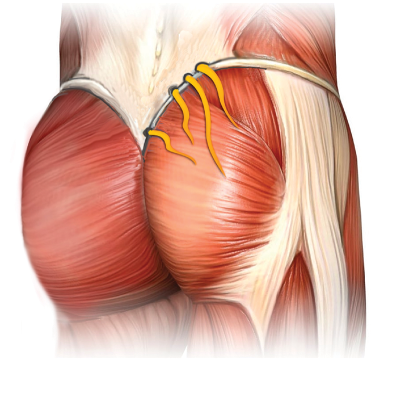
Branches of the superior cluneal nerve run from the spine through small fascial tunnels over the top of the pelvic brim and down toward the upper buttock (Image 4). Due to their location, I’ve been guilty of accidentally sliding an elbow up on the pelvic brim and squashing the nerves when performing low-back work.
Eventually, I figured out a better way to treat clients with low-back stiffness without intruding on the cluneal nerves. Notice how I use my right olecranon (Image 5) to push the tissue medial to lateral while resisting this motion with my left hand. This offers a nice stretch and allows the elbow to glide through the tissue and open the tunnels with greater precision.

the lumbar tissue medial to lateral while my left hand resists this effort.
Conclusion
Using the techniques outlined here can help us avoid eliciting the dreaded jump reflex or yelp that occurs when we accidentally collide with a client’s nerve. There are, of course, several other areas where it’s possible to “get on your client’s nerves,” and I sincerely hope you haven’t discovered any of them yet. To help you steer clear of sensitive spots in general, here are my three take-home messages: (1) be innovative when positioning clients on the therapy table, (2) use movement enhancers to calm the nervous system, and (3) don’t chase the pain.


